
Follow Brian on Twitter:
A PDF of this retracted paper is here
RETRACTED: Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children
A J Wakefield, S H Murch, A Anthony, J Linnell, D M Casson, M Malik, M Berelowitz, A P Dhillon, M A Thomson, P Harvey, A Valentine, S E Davies, J A Walker-Smith
The Lancet, Volume 351, Number 9103, 28 February 1998
Inflammatory Bowel Disease Study Group, University Departments of Medicine and Histopathology (A J Wakefield FRCS, A Anthony MB, J Linnell PhD, A P Dhillon MRCPath, S E Davies MRCPath) and the University Departments of Paediatric Gastroenterology (S H Murch MB, D M Casson MRCP, M Malik MRCP, M A Thomson FRCP, J A Walker-Smith FRCP,), Child and Adolescent Psychiatry (M Berelowitz FRCPsych), Neurology (P Harvey FRCP), and Radiology (A Valentine FRCR), Royal Free Hospital and School of Medicine, London NW3 2QG, UK
Correspondence to: Dr A J Wakefield
Summary
Background We investigated a consecutive series of children with chronic enterocolitis and regressive developmental disorder.
Methods 12 children (mean age 6 years [range 3-10], 11 boys) were referred to a paediatric gastroenterology unit with a history of normal development followed by loss of acquired skills, including language, together with diarrhoea and abdominal pain. Children underwent gastroenterological, neurological, and developmental assessment and review of developmental records. Ileocolonoscopy and biopsy sampling, magnetic-resonance imaging (MRI), electroencephalography (EEG), and lumbar puncture were done under sedation. Barium follow-through radiography was done where possible. Biochemical, haematological, and immunological profiles were examined.
Findings Onset of behavioural symptoms was associated, by the parents, with measles, mumps, and rubella vaccination in eight of the 12 children, with measles infection in one child, and otitis media in another. All 12 children had intestinal abnormalities, ranging from lymphoid nodular hyperplasia to aphthoid ulceration. Histology showed patchy chronic inflammation in the colon in 11 children and reactive ileal lymphoid hyperplasia in seven, but no granulomas. Behavioural disorders included autism (nine), disintegrative psychosis (one), and possible postviral or vaccinal encephalitis (two). There were no focal neurological abnormalities and MRI and EEG tests were normal. Abnormal laboratory results were significantly raised urinary methylmalonic acid compared with age-matched controls (p=0·003), low haemoglobin in four children, and a low serum IgA in four children.
Interpretation We identified associated gastrointestinal disease and developmental regression in a group of previously normal children, which was generally associated in time with possible environmental triggers.
Lancet 1998; 351: 637-41
Introduction
We saw several children who, after a period of apparent normality, lost acquired skills, including communication. They all had gastrointestinal symptoms, including abdominal pain, diarrhoea, and bloating and, in some cases, food intolerance. We describe the clinical findings, and gastrointestinal features of these children.
Patients and methods
12 children, consecutively referred to the department of paediatric gastroenterology with a history of a pervasive developmental disorder with loss of acquired skills and intestinal symptoms (diarrhoea, abdominal pain, bloating and food intolerance), were investigated. All children were admitted to the ward for 1 week, accompanied by their parents.
Clinical investigations
We took histories, including details of immunisations and exposure to infectious diseases, and assessed the children. In 11 cases the history was obtained by the senior clinician (JW-S). Neurological and psychiatric assessments were done by consultant staff (PH, MB) with HMS-4 criteria.1 Developmental histories included a review of prospective developmental records from parents, health visitors, and general practitioners. Four children did not undergo psychiatric assessment in hospital; all had been assessed professionally elsewhere, so these assessments were used as the basis for their behavioural diagnosis.
After bowel preparation, ileocolonoscopy was performed by SHM or MAT under sedation with midazolam and pethidine. Paired frozen and formalin-fixed mucosal biopsy samples were taken from the terminal ileum; ascending, transverse, descending, and sigmoid colons, and from the rectum. The procedure was recorded by video or still images, and were compared with images of the previous seven consecutive paediatric colonoscopies (four normal colonoscopies and three on children with ulcerative colitis), in which the physician reported normal appearances in the terminal ileum. Barium follow-through radiography was possible in some cases.
Also under sedation, cerebral magnetic-resonance imaging (MRI), electroencephalography (EEG) including visual, brain stem auditory, and sensory evoked potentials (where compliance made these possible), and lumbar puncture were done.
Laboratory investigations
Thyroid function, serum long-chain fatty acids, and cerebrospinal-fluid lactate were measured to exclude known causes of childhood neurodegenerative disease. Urinary methylmalonic acid was measured in random urine samples from eight of the 12 children and 14 age-matched and sex-matched normal controls, by a modification of a technique described previously.2 Chromatograms were scanned digitally on computer, to analyse the methylmalonic-acid zones from cases and controls. Urinary methylmalonic-acid concentrations in patients and controls were compared by a two-sample t test. Urinary creatinine was estimated by routine spectrophotometric assay.
Children were screened for antiendomyseal antibodies and boys were screened for fragile-X if this had not been done before. Stool samples were cultured for Campylobacter spp, Salmonella spp, and Shigella spp and assessed by microscopy for ova and parasites. Sera were screened for antibodies to Yersinia enterocolitica.
Histology
Formalin-fixed biopsy samples of ileum and colon were assessed and reported by a pathologist (SED). Five ileocolonic biopsy series from age-matched and site-matched controls whose reports showed histologically normal mucosa were obtained for comparison. All tissues were assessed by three other clinical and experimental pathologists (APD, AA, AJW).
Ethical approval and consent
Investigations were approved by the Ethical Practices Committee of the Royal Free Hospital NHS Trust, and parents gave informed consent.
Results
Clinical details of the children are shown in tables 1 and 2. None had neurological abnormalities on clinical examination; MRI scans, EEGs, and cerebrospinal-fluid profiles were normal; and fragile X was negative. Prospective developmental records showed satisfactory achievement of early milestones in all children. The only girl (child number eight) was noted to be a slow developer compared with her older sister. She was subsequently found to have coarctation of the aorta. After surgical repair of the aorta at the age of 14 months, she progressed rapidly, and learnt to talk. Speech was lost later. Child four was kept under review for the first year of life because of wide bridging of the nose. He was discharged from follow-up as developmentally normal at age 1 year.
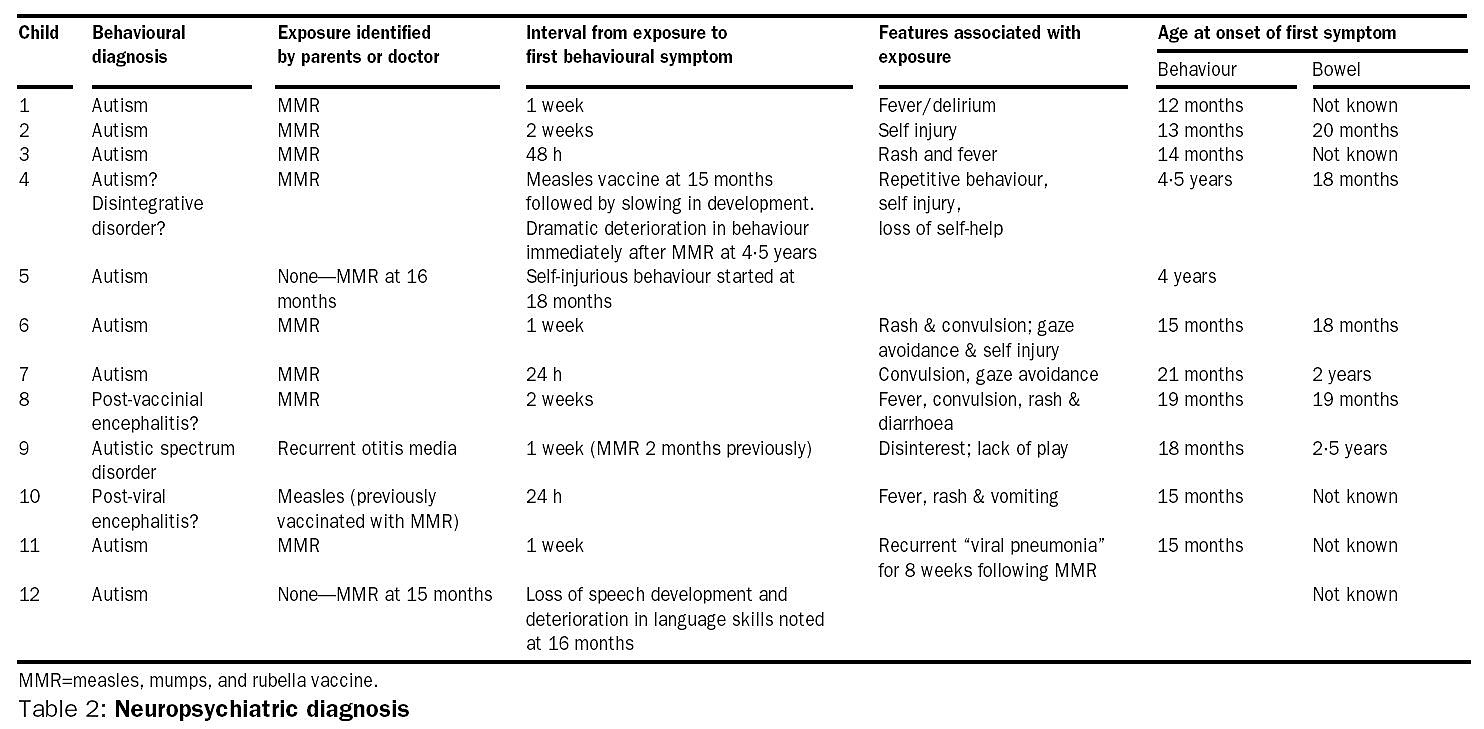
In eight children, the onset of behavioural problems had been linked, either by the parents or by the child’s physician, with measles, mumps, and rubella vaccination. Five had had an early adverse reaction to immunisation (rash, fever, delirium; and, in three cases, convulsions). In these eight children the average interval from exposure to first behavioural symptoms was 6·3 days (range 1-14). Parents were less clear about the timing of onset of abdominal symptoms because children were not toilet trained at the time or because behavioural features made children unable to communicate symptoms.
One child (child four) had received monovalent measles vaccine at 15 months, after which his development slowed (confirmed by professional assessors). No association was made with the vaccine at this time. He received a dose of measles, mumps, and rubella vaccine at age 4·5 years, the day after which his mother described a striking deterioration in his behaviour that she did link with the immunisation. Child nine received measles, mumps, and rubella vaccine at 16 months. At 18 months he developed recurrent antibiotic-resistant otitis media and the first behavioural symptoms, including disinterest in his sibling and lack of play.
Table 2 summarises the neuropsychiatric diagnoses; the apparent precipitating events; onset of behavioural features; and age of onset of both behaviour and bowel symptoms.
Table 1: Clinical details and laboratory, endoscopic, and histological findings
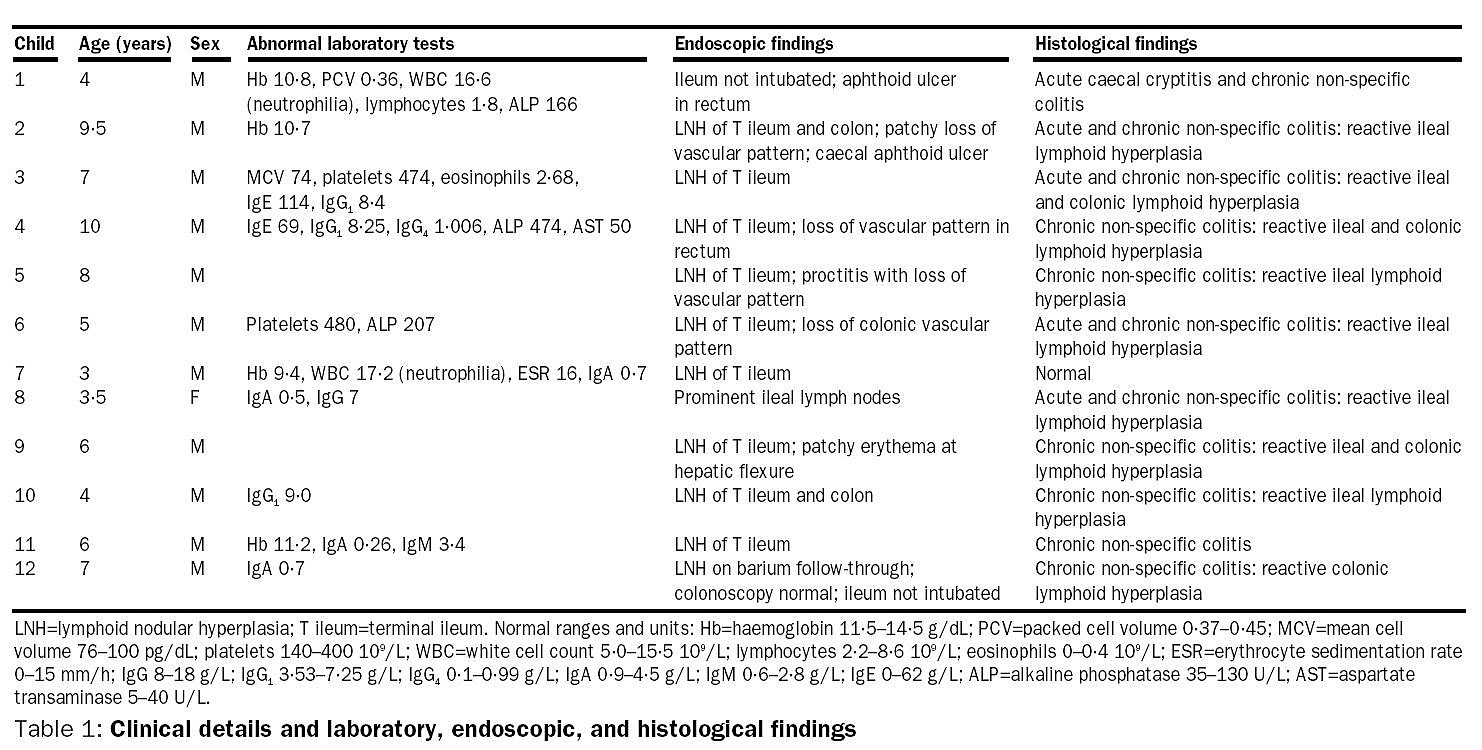
Table 2: Neuropsychiatric diagnosis
Laboratory tests
All children were antiendomyseal-antibody negative and common enteric pathogens were not identified by culture, microscopy, or serology. Urinary methylmalonic-acid excretion was significantly raised in all eight children who were tested, compared with age-matched controls (p=0·003; figure 1). Abnormal laboratory tests are shown in table 1.
Endoscopic findings
The caecum was seen in all cases, and the ileum in all but two cases. Endoscopic findings are shown in table 1. Macroscopic colonic appearances were reported as normal in four children. The remaining eight had colonic and rectal mucosal abnormalities including granularity, loss of vascular pattern, patchy erythema, lymphoid nodular hyperplasia, and in two cases, aphthoid ulceration. Four cases showed the “red halo” sign around swollen caecal lymphoid follicles, an early endoscopic feature of Crohn’s disease.3 The most striking and consistent feature was lymphoid nodular hyperplasia of the terminal ileum which was seen in nine children (figure 2), and identified by barium follow-through in one other child in whom the ileum was not reached at endoscopy. The normal endoscopic appearance of the terminal ileum (figure 2) was seen in the seven children whose images were available for comparison. [note: figures 1 – 3 are omitted from this online version]
Histological findings
Histological findings are summarised in table 1.
Terminal ileum A reactive lymphoid follicular hyperplasia was present in the ileal biopsies of seven children. In each case, more than three expanded and confluent lymphoid follicles with reactive germinal centres were identified within the tissue section (figure 3). There was no neutrophil infiltrate and granulomas were not present.
Colon The lamina propria was infiltrated by mononuclear cells (mainly lymphocytes and macrophages) in the colonic-biopsy samples. The extent ranged in severity from scattered focal collections of cells beneath the surface epithelium (five cases) to diffuse infiltration of the mucosa (six cases). There was no increase in intraepithelial lymphocytes, except in one case, in which numerous lymphocytes had infiltrated the surface epithelium in the proximal colonic biopsies. Lymphoid follicles in the vicinity of mononuclear-cell infiltrates showed enlarged germinal centres with reactive changes that included an excess of tingible body macrophages.
There was no clear correlation between the endoscopic appearances and the histological findings; chronic inflammatory changes were apparent histologically in endoscopically normal areas of the colon. In five cases there was focal acute inflammation with infiltration of the lamina propria by neutrophils; in three of these, neutrophils infiltrated the caecal (figure 3) and rectal-crypt epithelium. There were no crypt abscesses. Occasional bifid crypts were noted but overall crypt architecture was normal. There was no goblet-cell depletion but occasional collections of eosinophils were seen in the mucosa. There were no granulomata. Parasites and organisms were not seen. None of the changes described above were seen in any of the normal biopsy specimens.
Discussion
We describe a pattern of colitis and ileal-lymphoid-nodular hyperplasia in children with developmental disorders. Intestinal and behavioural pathologies may have occurred together by chance, reflecting a selection bias in a self-referred group; however, the uniformity of the intestinal pathological changes and the fact that previous studies have found intestinal dysfunction in children with autistic-spectrum disorders, suggests that the connection is real and reflects a unique disease process.
Asperger first recorded the link between coeliac disease and behavioural psychoses.4 Walker-Smith and colleagues5 detected low concentrations of alpha-1 antitrypsin in children with typical autism, and D’Eufemia and colleagues6 identified abnormal intestinal permeability, a feature of small intestinal enteropathy, in 43% of a group of autistic children with no gastrointestinal symptoms, but not in matched controls. These studies, together with our own, including evidence of anaemia and IgA deficiency in some children, would support the hypothesis that the consequences of an inflamed or dysfunctional intestine may play a part in behavioural changes in some children.
The “opioid excess” theory of autism, put forward first by Panksepp and colleagues7 and later by Reichelt and colleagues8 and Shattock and colleagues9 proposes that autistic disorders result from the incomplete breakdown and excessive absorption of gut-derived peptides from foods, including barley, rye, oats, and caesin from milk and dairy produce. These peptides may exert central-opioid effects, directly or through the formation of ligands with peptidase enzymes required for breakdown of endogenous central-nervous-system opioids,9 leading to disruption of normal neuroregulation and brain development by endogenous encephalins and endorphins.
One aspect of impaired intestinal function that could permit increased permeability to exogenous peptides is deficiency of the phenyl-sulphur-transferase systems, as described by Waring.10 The normally sulphated glycoprotein matrix of the gut wall acts to regulate cell and molecular trafficking.11 Disruption of this matrix and increased intestinal permeability, both features of inflammatory bowel disease,17 may cause both intestinal and neuropsychiatric dysfunction. Impaired enterohepatic sulphation and consequent detoxification of compounds such as the phenolic amines (dopamine, tyramine, and serotonin)12 may also contribute. Both the presence of intestinal inflammation and absence of detectable neurological abnormality in our children are consistent with an exogenous influence upon cerebral function. Lucarelli’s observation that after removal of a provocative enteric antigen children achieved symptomatic behavioural improvement, suggests a reversible element in this condition.13
Despite consistent gastrointestinal findings, behavioural changes in these children were more heterogeneous. In some cases the onset and course of behavioural regression was precipitous, with children losing all communication skills over a few weeks to months. This regression is consistent with a disintegrative psychosis (Heller’s disease), which typically occurs when normally developing children show striking behaviour changes and developmental regression, commonly in association with some loss of coordination and bowel or bladder function.14 Disintegrative psychosis is typically described as occurring in children after at least 2-3 years of apparently normal development.
Disintegrative psychosis is recognised as a sequel to measles encephalitis, although in most cases no cause is ever identified.14 Viral encephalitis can give rise to autistic disorders, particularly when it occurs early in life.15 Rubella virus is associated with autism and the combined measles, mumps, and rubella vaccine (rather than monovalent measles vaccine) has also been implicated. Fudenberg16 noted that for 15 of 20 autistic children, the first symptoms developed within a week of vaccination. Gupta17 commented on the striking association between measles, mumps, and rubella vaccination and the onset of behavioural symptoms in all the children that he had investigated for regressive autism. Measles virus18,19 and measles vaccination20 have both been implicated as risk factors for Crohn’s disease and persistent measles vaccine-strain virus infection has been found in children with autoimmune hepatitis.21
We did not prove an association between measles, mumps, and rubella vaccine and the syndrome described. Virological studies are underway that may help to resolve this issue.
If there is a causal link between measles, mumps, and rubella vaccine and this syndrome, a rising incidence might be anticipated after the introduction of this vaccine in the UK in 1988. Published evidence is inadequate to show whether there is a change in incidence22 or a link with measles, mumps, and rubella vaccine.23 A genetic predisposition to autistic-spectrum disorders is suggested by over-representation in boys and a greater concordance rate in monozygotic than in dizygotic twins.15 In the context of susceptibility to infection, a genetic association with autism, linked to a null allele of the complement (C) 4B gene located in the class III region of the major-histocompatibility complex, has been recorded by Warren and colleagues.24 C4B-gene products are crucial for the activation of the complement pathway and protection against infection: individuals inheriting one or two C4B null alleles may not handle certain viruses appropriately, possibly including attenuated strains.
Urinary methylmalonic-acid concentrations were raised in most of the children, a finding indicative of a functional vitamin B12 deficiency. Although vitamin B12 concentrations were normal, serum B12 is not a good measure of functional B12 status.25 Urinary methylmalonic-acid excretion is increased in disorders such as Crohn’s disease, in which cobalamin excreted in bile is not reabsorbed. A similar problem may have occurred in the children in our study. Vitamin B12 is essential for myelinogenesis in the developing central nervous system, a process that is not complete until around the age of 10 years. B12 deficiency may, therefore, be a contributory factor in the developmental regression.26
We have identified a chronic enterocolitis in children that may be related to neuropsychiatric dysfunction. In most cases, onset of symptoms was after measles, mumps, and rubella immunisation. Further investigations are needed to examine this syndrome and its possible relation to this vaccine.
Addendum:
Up to Jan 28, a further 40 patients have been assessed; 39 with the syndrome.
Contributors
A J Wakefield was the senior scientific investigator. S H Murch and M A Thomson did the colonoscopies. A Anthony, A P Dhillon, and S E Davies carried out the histopathology. J Linnell did the B12 studies. D M Casson and M Malik did the clinical assessment. M Berelowitz did the psychiatric assessment. P Harvey did the neurological assessment. A Valentine did the radiological assessment. JW-S was the senior clinical investigator.
Acknowledgments
This study was supported by the Special Trustees of Royal Free Hampstead NHS Trust and the Children’s Medical Charity. We thank Francis Moll and the nursing staff of Malcolm Ward for their patience and expertise; the parents for providing the impetus for these studies; and Paula Domizo, Royal London NHS Trust, for providing control tissue samples.
References
1 Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). 4th edn. Washington DC, USA: American Psychiatric Association, 1994.
2 Bhatt HR, Green A, Linnell JC. A sensitive micromethod for the routine estimations of methylmalonic acid in body fluids and tissues using thin-layer chromatography. Clin Chem Acta 1982; 118: 311-21.
3 Fujimura Y, Kamoni R, Iida M. Pathogenesis of aphthoid ulcers in Crohn’s disease: correlative findings by magnifying colonoscopy, electromicroscopy, and immunohistochemistry. Gut 1996; 38: 724-32.
4 Asperger H. Die Psychopathologie des coeliakakranken kindes. Ann Paediatr 1961; 197: 146-51.
5 Walker-Smith JA, Andrews J. Alpha-1 antitrypsin, autism and coeliac disease. Lancet 1972; ii: 883-84.
6 D’Eufemia P, Celli M, Finocchiaro R, et al. Abnormal intestinal permeability in children with autism. Acta Paediatrica 1996; 85: 1076-79.
7 Panksepp J. A neurochemical theory of autism. Trends Neurosci 1979; 2: 174-77.
8 Reichelt KL, Hole K, Hamberger A, et al. Biologically active peptide-containing fractions in schizophrenia and childhood autism. Adv Biochem Psychopharmacol 1993; 28: 627-43.
9 Shattock P, Kennedy A, Rowell F, Berney TP. Role of neuropeptides in autism and their relationships with classical neurotransmitters. Brain Dysfunction 1991; 3: 328-45.
10 Waring RH, Ngong JM. Sulphate metabolism in allergy induced autism: relevance to disease aetiology, conference proceedings, biological perspectives in autism, University of Durham, NAS 35-44.
11 Murch SH, MacDonald TT, Walker-Smith JA, Levin M, Lionetti P, Klein NJ. Disruption of sulphated glycosaminoglycans in intestinal inflammation. Lancet 1993; 341: 711-41.
12 Warren RP, Singh VK. Elevated serotonin levels in autism: association with the major histocompatibility complex. Neuropsychobiology 1996; 34: 72-75.
13 Lucarelli S, Frediani T, Zingoni AM, et al. Food allergy and infantile autism. Panminerva Med 1995; 37: 137-41.
14 Rutter M, Taylor E, Hersor L. In: Child and adolescent psychiatry. 3rd edn. London: Blackwells Scientific Publications: 581-82.
15 Wing L. The Autistic Spectrum. London: Constable, 1996: 68-71.
16 Fudenberg HH. Dialysable lymphocyte extract (DLyE) in infantile onset autism: a pilot study. Biotherapy 1996; 9: 13-17.
17 Gupta S. Immunology and immunologic treatment of autism. Proc Natl Autism Assn Chicago 1996; 455-60.
18 Miyamoto H, Tanaka T, Kitamoto N, Fukada Y, Takashi S. Detection of immunoreactive antigen with monoclonal antibody to measles virus in tissue from patients with Crohn’s disease. J Gastroenterol 1995; 30: 28-33.
19 Ekbom A, Wakefield AJ, Zack M, Adami H-O. Crohn’s disease following early measles exposure. Lancet 1994; 344: 508-10.
20 Thompson N, Montgomery S, Pounder RE, Wakefield AJ. Is measles vaccination a risk factor for inflammatory bowel diseases? Lancet 1995; 345: 1071-74.
21 Kawashima H, Mori T, Takekuma K, Hoshika A, Hata A, Nakayama T. Polymerase chain reaction detection of the haemagglutinin gene from an attenuated measles vaccines strain in the peripheral mononuclear cells of children with autoimmune hepatitis. Arch Virol 1996; 141: 877-84.
22 Wing L. Autism spectrum disorders: no evidence for or against an increase in prevalence. BMJ 1996; 312: 327-28.
23 Miller D, Wadsworth J, Diamond J, Ross E. Measles vaccination and neurological events. Lancet 1997; 349: 730-31.
24 Warren RP, Singh VK, Cole P, et al. Increased frequency of the null allele at the complement C4B locus in autism. Clin Exp Immunol 1991; 83: 438-40.
25 England JM, Linnell JC. Problems with the serum vitamin B12 assay. Lancet 1980; ii: 1072-74.
26 Dillon MJ, England JM, Gompertz D, et al. Mental retardation, megaloblastic anaemic, homocysteine metabolism due to an error in B12 metabolism. Clin Sci Mol Med 1974; 47: 43-61.
A PDF of this retracted paper is here
Follow Brian on Twitter:
RELATED:
Vexatious Wakefield lawsuits fail