
Wakefield swollen glands reported before MMR was licensed
In February 1998, a worldwide scare was launched over the safety of the MMR children’s vaccine with a paper in The Lancet by Andrew Wakefield and others, titled “Ileal-lymphoid-nodular hyperplasia, non-specific colitis and pervasive developmental disorder in children”.
Get Deer’s book: The Doctor Who Fooled the World
This hyperplasia sounds terrible, and looks even worse, leading many to think that Wakefield had discovered – as he claimed – a new bowel condition in children, associated with autism and MMR. Surprisingly, the paper included no discussion, explanation of this hyperplasia, or any references to previous literature. Here’s (some of) what Wakefield didn’t tell us:

Endoscopic view of ileal-lymphoid nodular hyperplasia
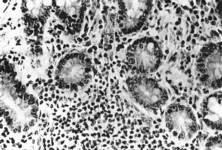 Microscopic section of ileal-lymphoid hyperplasia biopsy (Walker-Smith et al, 1983)
Microscopic section of ileal-lymphoid hyperplasia biopsy (Walker-Smith et al, 1983)
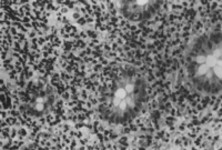
Microscopic section of ileal-lymphoid hyperplasia biopsy (Wakefield et al, 1998)
Practical Paediatric Gastroenterology.
J A Walker-Smith, J R Hamilton, W A Walker. Butterworths. 1983
Lymphoid hyperplasia
“The last form of NLH is that restricted to the terminal ileum which has also been termed benign lymphoid hyperplasia due to the frequency of its demonstration in asymptomatic children. While particularly frequent in adolescents, it has also been seen in infancy and in the elderly. Recurrent abdominal pain and diarrhoea often prompt the diagnostic small bowel contrast studies although the association of such symptoms with ileal NLH is all too often circumstantial. Histologically, discrete polypoid lesions of lymphoid tissue with germinal centres are present. These polyps may be pedunculated and eosinophils are often prominent.”
Selective Biopsy of Human Peyer’s Patches During Ileal Endoscopy.
Thomas T MacDonald, Jo Spencer, Joanne L Viney, Christopher B Williams, and John A Walker-Smith. Gastroenterology 1987; 93: 1356-62
Get Deer’s book: The Doctor Who Fooled the World
“During routine diagnostic colonoscopy of children, it is possible to reach as far as the last few centimeters of the terminal ileum in 90% of the patients. Lymphoid follicles (PPs) are frequently seen, especially in younger children.”
“The typical appearance of the terminal ileum in a child is shown in Figure 1. The PPs are clearly identifiable as whitish blebs protruding above the rest of the mucosa.”
“Peyer’s patches are more numerous in the ileum of children and are clearly visible through the colonoscope.”
Endoscopic features of chronic inflammatory bowel disease in childhood.
Christopher B Williams and Stuart Nicholls. In Bailliere’s Clinical Gastroenterology, Vol 8/Number 1, March 1994, edited by J A Walker-Smith and T T MacDonald
Lymphoid nodular hyperplasia (LNH)
“This entity of uncertain clinical significance has been found in 24% of barium follow-through examinations when investigating for suspected childhood chronic IBD, and has caused diagnostic confusion between Crohn’s disease and LNH. Shiny subepithelial 1mm nodules of lymphatic tissue may be found throughout the colon, being most conspicuous in children under 5 years of age and after infective episodes. The most characteristic and clinically important appearance is in the terminal ileum, where 1-5mm nodules, usually pink and shiny, but sometimes matt-surfaced, pale or even yellowish, can be dotted around singly or as coalescing masses. Localized conglomerations around 10-15mm diameter are described as Peyer’s patches.”
Radiological investigation of chronic inflammatory bowel disease in childhood.
C I Bartram and S Halligan. In Bailliere’s Clinical Gastroenterology, Vol 8/Number 1, March 1994, edited by J A Walker-Smith and T T MacDonald
“Lymphoid hyperplasia in the terminal ileum is an important differential diagnosis. This is so common as to be a normal variant in children. Enlargement of the submucosal lymphoid follicles creates a nodular pattern with regular 2mm defects deforming the thin barium-filled parallel folds that are seen in the contracted ileum. More pronounced lymphoid hyperplasia involves the Peyer’s patches. Enlargement of these causes a disorganized fold pattern as the linear contracted pattern is obliterated rather than just deformed. Compression views are invaluable to exclude ulceration and the appearance must not be confused with Crohn’s disease.”
Children reported on above were not recorded as having any behavioural disorders. Nevertheless many parents were tricked into believing Wakefield had discovered a new condition, linked to autism.
Get Deer’s book: The Doctor Who Fooled the World
Even the British Medical Journal wrongly noted, on March 7 1998, with regard to Wakefield’s now-infamous Lancet publication of February 28:
“The study is the first of five new papers to be published on the new syndrome, which the team have named ileal lymphoid nodular hyperplasia.”
RELATED:
Vexatious Wakefield lawsuits fail